An ‘Expert Panel’ is Not Good Enough – We Need to Re-Schedule Cannabis

The Home Office today announced the details of an expert panel which will take clinical applications for medical cannabis licenses. While we welcome a legal pathway for patients to access their medication, this does not address a key issue – that the Home Office still insists on micro-managing the medical affairs of individuals who shouldn’t be under their jurisdiction in the first place.
It is hard not to be moved by the story of Charlotte Caldwell, Hannah Deacon, and the other parents who have spent years watching their children suffer as an implacable wall of bureaucracy stands between them and their medicine.
Those who ignore their plight are often individuals who maintain that wall. Following a public campaign earlier this year, Prime Minister Theresa May personally assured Hannah Deacon, mother of Alfie Dingley, that her application for a cannabis license would be rapidly processed if she withdrew from the media spotlight. Immediately after her story left the papers, Hannah was roundly disregarded, her licence application ignored, and Theresa May refused to acknowledge the issue.
Were it not for Charlotte Caldwell propelling herself into the public perception and bringing cannabis policy back onto the political radar, it’s likely Alfie’s licence would never have been processed.
In the face of overwhelming public pressure from Charlotte’s campaign, Sajid Javid did well in acting swiftly. But returning Billy Caldwell’s medicine and granting Alfie Dingley a license using “exceptional powers as Home Secretary” assumes that it was unexceptional for the Home Office to interfere with a family’s medical affairs in the first place.
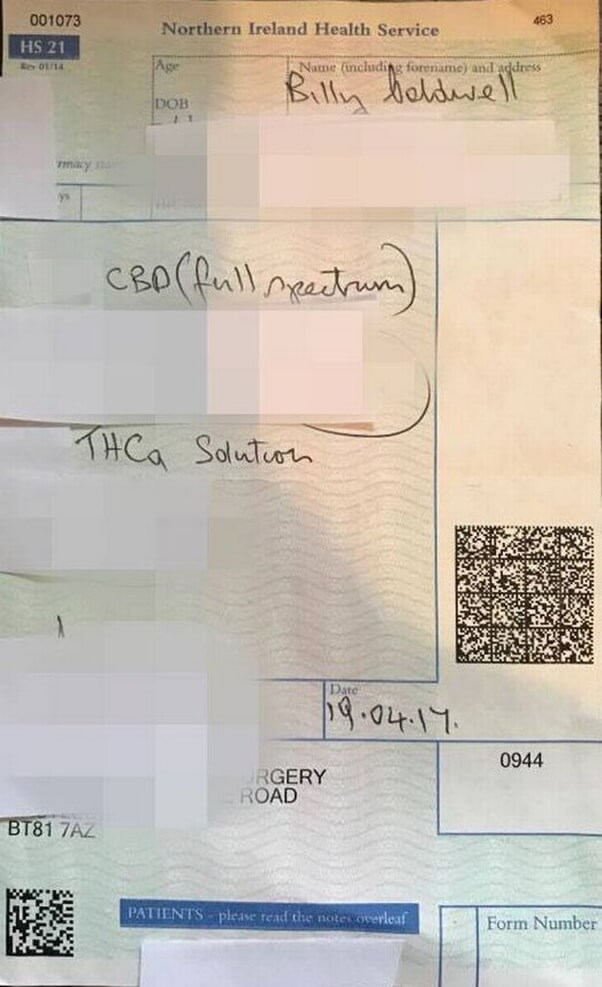
Billy Caldwell’s original cannabis oil prescription, the first and only on the NHS, which was rapidly over-ruled by the Home Office
We don’t see a prescribed medicine being given to a patient as requiring exceptional political powers. Indeed, it is exceptional political over-reach which saw Billy Caldwell’s cannabis prescription – previously fulfilled by a pharmacy in Northern Ireland – blocked by the Home Office, and which sees politicians systematically over-ride medical decisions made by doctors.
The announcement by the Home Office of a new expert panel that will take applications for cannabis licences is a step in the right direction, in that it at least offers a legal pathway for patients to access a necessary medication. Yet this action also seems suspiciously like the bare minimum the Home Office was willing to concede in the face of overwhelming public pressure.
This panel will take two to four weeks to assess individual patients – far too long when patients have a life-threatening condition which sees them have dozens of seizures every day. Furthermore, it is unrealistic to expect that individuals be assessed on a case-by-case basis when there are between 30,000 and 1,000,000 people using medical cannabis in the U.K.
It is perhaps natural that the Home Office – a bureau tasked with security and immigration – performs its functions in a way that assumes wrong-doing on the part of the individuals under their jurisdiction, necessitating micro-management and close scrutiny by a central bureaucracy.
The Home Office may believe it can regulate patients in the same way it regulates cannabis-exporting corporations, by granting a couple of licences a week. They may also genuinely believe that the only individuals who require medicinal cannabis are those that make the front pages.
The reality is that the Home Office is utterly unequipped to handle social health policy. The prescription of drugs, taking into consideration the individual nuance and medical history of each individual, is a decentralised decision that needs to be made by one’s doctor. The expert panel’s own prerequisite that applications come from “senior clinicians with expertise in your condition” should be the end-point of the application, not the entry to a bottleneck.

Products from Tilray.CA, the company now providing Billy Caldwell’s cannabis oil
This is further complicated by the fact that, due to current restrictions on medical cannabis, senior clinicians for cannabis medicines don’t exist. And any doctors who wish to engage with them may be nervous about the Home Office scrutinizing their decisions. In a recent press release, Charlotte Caldwell rightly asks: what guidance will be offered to GP’s who have no experience or knowledge of cannabis? What will be the penalties for clinicians who contravene any regulations?
“It feels to us and to the vast majority of our patients that this process is written more to limit and manage the number of applications, than to provide an effective service for patients,” says Jon Liebling of United Patients Alliance, an advocacy group representing 5,000 medical cannabis users. “We hope that a more patient-centred approach is used in determining broader policy on cannabis as medicine.”
The most pragmatic policy action that the Home Office should immediately take, one that will most benefit doctors and patients, is to re-schedule cannabis and cannabinoid derivatives from Schedule I to Schedule II. This would allow medical professionals to use their discretion in treating their patients – a move which has been urged by a host of experts, including our collaborators Prof. David Nutt and Prof. Celia Morgan.
“The U.S. and other European countries have shown that implementing access to medical cannabis is not only plausible, but beneficial” writes Amanda Feilding, director of the Beckley Foundation and convener of the Global Cannabis Commission. “It is about time our wonderful country once again takes a lead in these matters.”
Nick Cherbanich



Podcast
- All
Links
- All
Support
- All
BIPRP
- All
Science Talk
- All
Amanda's Talks
- All
- Video Talk
- Featured
- 2016 Onwards
- 2011-2015
- 2010 and Earlier
- Science Talk
- Policy Talk
One-pager
- All
Music
- All
Amanda Feilding
- All
Events
- All
Highlights
- All
Psilocybin for Depression
- All
Current
- All
Category
- All
- Science
- Policy
- Culture
Substance/Method
- All
- Opiates
- Novel Psychoactive Substances
- Meditation
- Trepanation
- LSD
- Psilocybin
- Cannabis/cannabinoids
- Ayahuasca/DMT
- Coca/Cocaine
- MDMA
Collaboration
- All
- Beckley/Brazil Research Programme
- Beckley/Maastricht Research Programme
- Exeter University
- ICEERS
- Beckley/Sant Pau Research Programme
- University College London
- New York University
- Cardiff University
- Madrid Computense University
- Ethnobotanicals Research Programme
- Freiburg University
- Medical Office for Psychiatry and Psychotherapy, Solothurn
- Beckley/Sechenov Institute Research programme
- Hannover Medical School
- Beckley/Imperial Research Programme
- King's College London
- Johns Hopkins University
Clinical Application
- All
- Depression
- Addictions
- Anxiety
- Psychosis
- PTSD
- Cancer
- Cluster Headaches
Policy Focus
- All
- Policy Reports
- Advisory Work
- Seminar Series
- Advocacy/Campaigns
Type of publication
- All
- Original research
- Report
- Review
- Opinion/Correspondence
- Book
- Book chapter
- Conference abstract
- Petition/campaign
Search type